By Mark D. Scholl, M.D — All cyclists know the joy of riding on the perfect day. Whether trails or road, gravel, or the flow of a downhill mountain track, when the weather is favorable and you find yourself pedaling circles with power to spare, you feel yourself energized in the moment. Many of us have seen our day quickly plummet to the other end of the spectrum, however. The dread cycling crash: a touch of wheels and hard to the tarmac, the mountain bike endo, an unexpected rock or pothole, or maybe a distracted driver. When that perfect day goes sideways, it becomes time to assess the damage. Some falls result in scrapes and bruises, losing skin and pride, but allow the day’s ride to continue. Other cycling crashes result in more significant injury. Breaking a bone from a fall is usually an injury that ends your day and often a good portion of your riding season. As with many sports, cycling fractures tend to show patterns due to the common mechanics of falling from a bicycle. As the bike loses its vertical positioning, the upper body accelerates to the ground at a high rate of speed resulting in over 85% of cycling fractures occurring in the upper body. The most common being a fracture of the clavicle / collarbone.
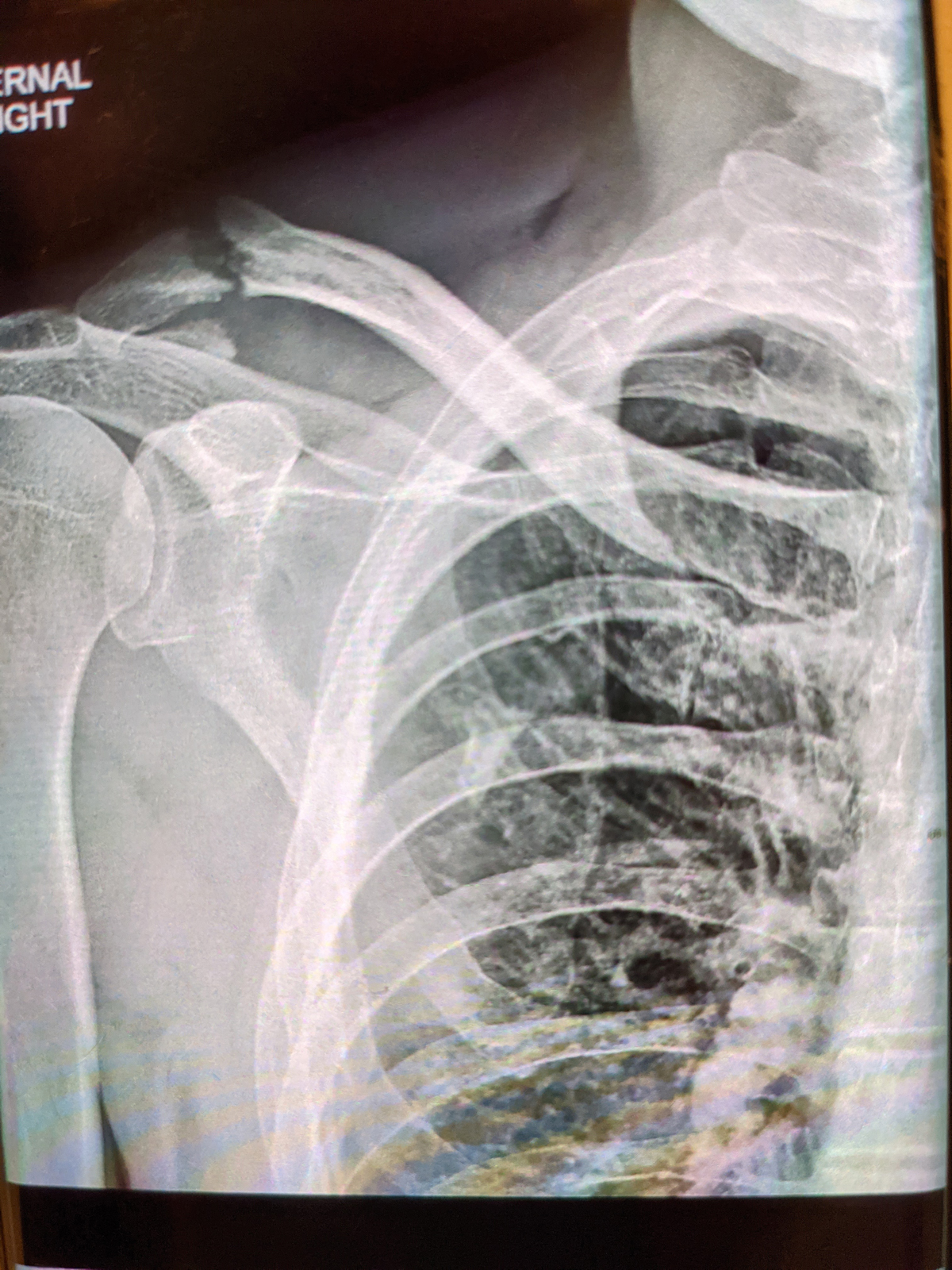
The clavicle is a doubly curved bone that connects the sternum to a projection of the shoulder blade called the acromion. Its primary function is acting as a strut to position the shoulder joint broadly outside the rib cage, to maximize function and range-of-motion. It derives its name from the Latin word “clavicula” which means “little key” because as the hand is taken above the head, the clavicle is seen to rotate on its long axis like a key in a lock.
Historically in medicine, fractures of the clavicle have been treated with limited intervention. Comfort measures such as a sling, or a figure-of-eight brace are used to help support the bone as the healing process occurs over time. Surgery was reserved for uncommon situations where the bone had broken through the skin, or was nearly through and was “tenting” the skin demonstrating significant stretch and risk of pressure injury developing. Traditional teaching instructed us that the vast majority of fractures would heal without intervention, often leaving a residual ‘bump’ but having no detrimental functional effect on the shoulder.
Over the past decade or so, orthopedic surgeons have begun to re-define what the effects of a clavicle fracture on a shoulder may be. It turns out our previous notion – that all patients who have a broken clavicle and successfully heal the bone go on to have full function of the shoulder without problems – may have been a bit shortsighted. Reports in the Journal of Bone and Joint Surgery (British & American versions) have begun to look at long-term outcomes after successful healing of displaced clavicle fractures. We have found that although these fractures often go on to heal, some patients with a healed fracture still have weakness or other functional limitations in the affected shoulder. Recent articles have shown that even at an average of 4.5 years after healing a displaced fracture of the clavicle, tested subjects were found to average around 80% strength in their shoulder compared to their uninjured side.
This loss of strength is, in most cases, the result of the loss of length to the clavicle. When the bone is fractured, the forces of the muscles which span from chest to shoulder (primarily the pectorals) cause compression of the broken bone, and it becomes shortened. Clavicle fractures have a high rate of healing in this shortened position, but it results in permanent change to the biomechanics and compromises the ability to generate strength. This is one of the main reasons orthopedic surgeons now treat many more fractures of the clavicle with surgery than we did even ten years ago.
The other reason we have begun to see orthopedic surgeons recommend treating clavicle fractures with surgery more often, has to do with the speed with which we can rehabilitate an athlete and return them to sport after surgery. Orthopedics has seen important advancements in the technology of devices available to stabilize clavicle fractures in surgery. As we are able to hold the fracture more securely, we can be more aggressive with our rehabilitation and get athletes back to sport much sooner than if we treat with immobilization and waiting. Most of the pain from a fracture comes from motion between the bones where there should not be any. Stabilizing the fracture with a plate and screws brings the bone ends together solidly, so there is no longer motion at the fracture site. This improves comfort much sooner, allowing early advancement in range-of-motion, sooner resumption of cardiovascular activities, and faster return to strengthening. All of these lead to faster return to sport.
The best clavicle is the one that was never broken, so using caution while riding, particularly in traffic or other adverse conditions, is always recommended. However, if you do have a crash and feel significant, focal pain around the clavicle or shoulder, it’s best to have it checked early by an orthopedic surgeon. Timing of treatment can make a difference and as with many medical problems, earlier diagnosis and formulation of treatment plan will lead to better results. We may be able to get you back in the saddle sooner than you think, and quite possibly with a better long-term outcome than a generation ago.
Mark D. Scholl, M.D. is an Orthopedic Sports Medicine Surgeon with Endurance Orthopedics & Sports Medicine. Information on his practice can be found online at Enduranceortho.com






{kind=link}
New and interesting news on clavicle fractures. Included should be the admonition to prevent breaks by learning to roll when you fall, not put out an arm to catch yourself. That is what generally breaks the clavicle. I will forever thank my elementary school PE teacher who had a great tumbling unit. I have fallen off horses and bikes and been hit by cars when running and on biking and have never broken a bone because I rolled. I am thankful for being lucky as well, but am positive that the ability to tuck and roll has saved a lot of breaks.
This article is good timing as I just broke mine at the 12 Hours at Pow Mow a couple weeks ago. I wonder if there is a general recommendation for athletes regarding eventual removal of the hardware?
Comments are closed.